

CLINICAL STUDIES
Background. Breast cancer is the most common cancer and the leading cause of cancer mortality among women. Determination of the molecular subtype is a key step in selecting the appropriate treatment strategy. Despite the standardization of current diagnostic methods, the risk of diagnostic errors remains significant, highlighting the need for noninvasive technologies that enable simultaneous assessment of tumor extent and HER2 expression.
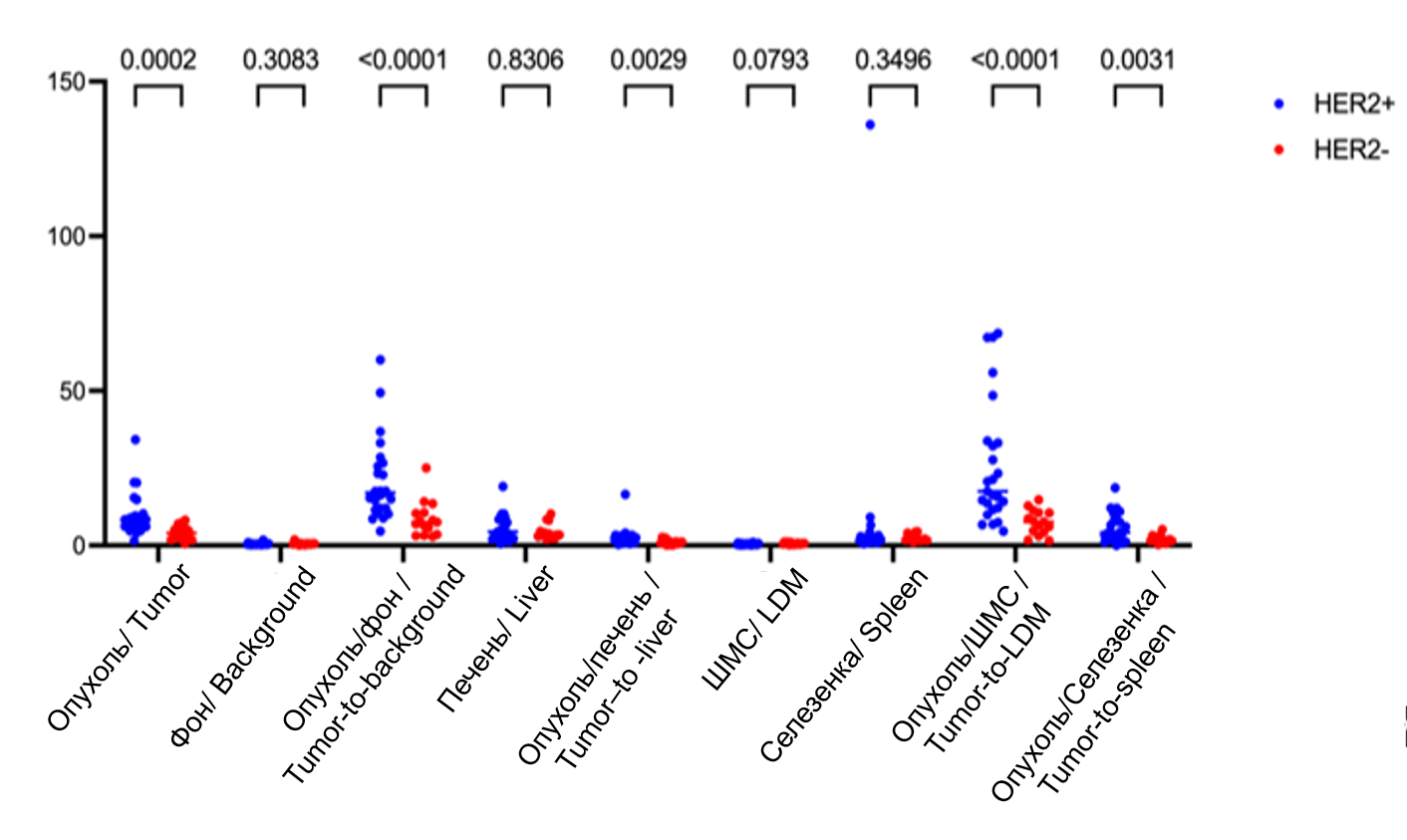
The purpose of study was to evaluate the feasibility of anatomical visualization and determination of the HER2 receptor status of primary breast tumors and malignant axillary lymph nodes (mAlN) using [99mTc]Tc-ADAPT6.
Material and Methods. The study included 40 patients with T2−4N1−3M0 breast cancer before starting systemic treatment. All patients underwent morphological and iHC studies of HER2 expression in tumors and mAlN (25 patients with positive and 15 patients with negative HER2 status). The patients were injected with 500 µg of [99mTc]Tc-ADAPT6 followed by SPECT/CT imaging 2 hours after injection. The accumulation of [99mTc]Tc-ADAPT6 was assessed by measuring the SUVmax in the primary breast tumor and the contralateral breast (background), as well as in mAlN and contralateral axillary region (background), the liver, the latissimus dorsi muscle (lDM) and the spleen. Tumor-to-reference organ and mAlN-to-reference organ ratios were also measured. Statistical data was calculated using Prism 10.2 for Windows.
Results. The findings demonstrated the feasibility of assessing locoregional disease extent and HER2 receptor status in the primary breast tumor and metastatic axillary lymph nodes using the radiopharmaceutical [99mTc]Tc-ADAPT6. The tumor-to-lDM ratio ≥11.46 relative units was the most informative parameter for differentiating HER2-positive from HER2-negative status in primary tumors (80 % sensitivity and 86 % specificity, p<0.0001). For metastatic axillary lymph nodes, the most informative parameters were the mAlNto-lDM ratio ≥4.470 relative units (p<0.0001) and the mAlN-to-spleen ratio ≥1.196 relative units (p<0.0001) with 88 % sensitivity and 86.67 % specificity.
Conclusion. The use of [99mTc]Tc-ADAPT6 in breast cancer patients enables assessment of locoregional disease extent and discrimination between HER2-positive and HER2-negative status in the primary tumor and metastatic axillary lymph nodes.

Objective: to assess whether shortening the time interval between transperineal prostate biopsy and laparoscopic radical prostatectomy (lRP) affects postoperative complications and early pathological outcomes.
Material and Methods. Prospective single-center randomized trial included 28 men with localized prostate cancer. Patients were assigned to two treatment groups: early lRP (n=9) performed 9–23 days after biopsy (median 14 days) and delayed lRP (n=19) performed 51–180 days after biopsy (median 105 days). The primary endpoint was complication-free survival (time from surgery to the first postoperative complication). Kaplan–Meier analysis (log-rank), Cox regression and exploratory prediction models were used.
Results. No statistically significant differences in baseline characteristics (age, BMi, PSA, prostate volume, comorbidities) between the treatment groups were found (p>0.05). Operative time was shorter in the early lRP group than in the delayed lRP (110 (85–230) min vs 145 (90–265) min, p=0.017), while blood loss was similar (150 (50–500) ml vs 150 (100–600) ml, p=0.37). Complications within 30 days occurred in 2 (22.2 %) vs 3 (15.8 %) (p=1.0); all events occurred on postoperative days 6–9 and none beyond day 30. Thirty-day complication-free survival was 77.8 % vs 84.2 % with no significant difference (log-rank p=0.648); Cox HR for immediate surgery was 1.50 (95 % Ci 0.25–8.96).
Conclusion. in this small randomized cohort, early lRP after transperineal biopsy showed no increase in complication rates and negative impact on pathological outcomes compared to delayed lRP. larger studies are required to confirm equivalence margins and evaluate long-term oncologic and functional outcomes.
The purpose of the study was to evaluate the effect of perioperative bronchodilator therapy on the incidence of postoperative complications and survival in non-small cell lung cancer (NSClC) patients with chronic obstructive pulmonary disease (COPD).
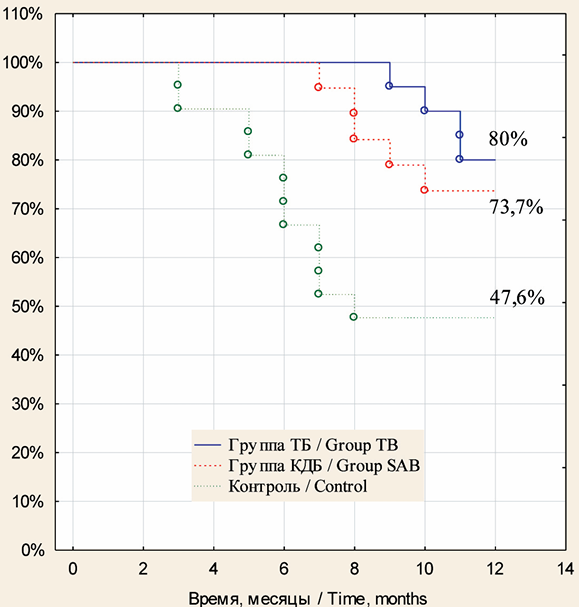
Material and Methods. The study included 66 patients with stage IВ–IIIА NSCLC and stage I–III COPD, who were divided into 3 groups. Group 1 consisted of 22 patients who received tiotropium bromide (a long-acting bronchodilator) for 6 weeks before and 6 weeks after surgery. Group 2 consisted of 21 patients, who received ipratropium bromide/fenoterol (a short-acting bronchodilator) for 6 weeks before and 6 weeks after surgery. Group 3 (control group) comprised 23 patients who received ipratropium bromide/fenoterol for 6 weeks after surgery. Patients of groups 1 and 2 received 2 courses of neoadjuvant carboplatin-based chemotherapy. All patients underwent radical surgery: lobectomy (47 %), bilobectomy (22.7 %) and pneumonectomy (30.3 %). Postoperative complications were classified according to the TMM system (2010). One-year survival was estimated using the Kaplan–Meier method; curve comparisons were performed using the log-rank test.
Results. Postoperative complications were observed in 9 (40.9 %), 14 (66.7 %) and 18 (78.3 %) patients of groups 1, 2 and 3, respectively. Significant statistical differences between group 1 and the control group were found (р˂0.05). The rate of grade ii postoperative respiratory complications was significantly lower in group 1 than in groups 2 and 3 (18.2 % vs 52.4 % and 65.2 %, respectively, р˂0.05). One-year relapse-free and overall survival rates were significantly higher in group 1 patients than in the control group (80 % vs 47.6 % (p=0.032) and 90 % vs 61.9 %, (p=0.037) respectively). In group 2 patients, the relapse-free and overall survival rates were lower than in group 1 patients, but were higher than in the control group (73.7 % (р=0.093) and 89.5 % (р=0.045), respectively).
Conclusion. In patients with NSClC and COPD, perioperative bronchodilator therapy with tiotropium bromide was more effective and associated with a lower incidence of postoperative pulmonary complications than ipratropium bromide/fenoterol therapy, and in combination with neoadjuvant chemotherapy contributed to improved survival rates. Long-term treatment results require further research.
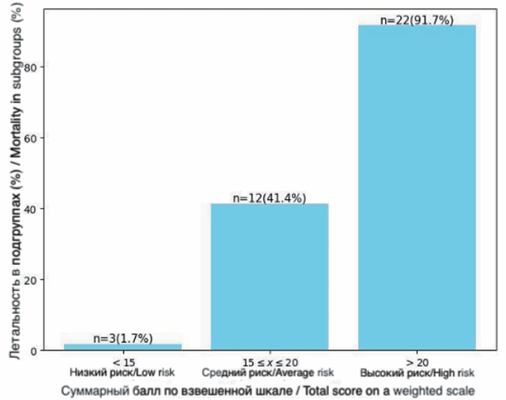
Objective: to develop a preoperative model for predicting 90-day mortality to optimize treatment strategy in patients with resectable esophageal cancer and Siewert type I gastroesophageal junction cancer.
Material and Methods. A retrospective cohort study included 225 patients with resectable esophageal cancer (n=179) and Siewert type I gastroesophageal junction cancer (n=46). A total of 79 preoperative variables were analyzed. Risk factors were selected using univariate and multivariate logistic regression. The dataset was randomly split into training and validation cohorts (70/30). The predictive model was developed using l1-regularized multivariable logistic regression and the TabNet neural network featuring a sparse attentive architecture that enables estimation of feature importance. Discriminative ability and calibration were assessed using AUCROC analysis and the Hosmer–Lemeshow test.
Results. The in-hospital mortality, 30-day mortality and 90-day mortality rates were 8.9 % (n=20), 1.3 % (n=3), and 6.2 % (n=14), respectively. The most significant predictors of mortality included preoperative weight loss >10 %, grade 3–4 dysphagia, ECOG performance status ≥2, COPD, preoperative dyspnea, history of major thoracic surgery, TNM stage N2, tumor proximity to or invasion of the trachea/main bronchi, cerebrovascular disease history, diabetes mellitus, and complications during or after radiotherapy. The logistic regression model demonstrated an AUC-ROC of 0.86 (95 % Ci 0.79–0.92) in the training cohort and 0.77 (95 % CI 0.72–0.83) in the validation cohort. Calibration was supported by non-significant Hosmer–Lemeshow χ2 tests in both cohorts: χ2=1.98, df=8 (p=0.98) and χ2=4.72, df=8 (p=0.78), respectively. The TabNet neural network achieved improved discrimination with AUC-ROC values of 0.95 (95 % CI 0.92–0.98) in the training cohort and 0.86 (95 % Ci 0.82–0.96) in the validation cohort; calibration results were χ2=8.38, df=8 (p=0.39) and χ2=9.46, df=8 (p=0.30), respectively. The model has been implemented as a software application and can be used in real-world clinical scenarios.
Conclusion. In this study, a machine learning-based model for preoperative 90-day mortality prediction was developed. It demonstrated good validity and high discriminative performance. The findings support the promise of machine learning methods for clinical risk prediction in cancer surgery and highlight their potential for implementation in routine healthcare practice.
Introduction. The melanocortin-1 receptor (MC1R) gene is one of the key factors in susceptibility to cutaneous melanoma (CM). The influence of specific germline MC1R polymorphisms on disease aggressiveness, tumor morphology, and patient survival has not been sufficiently studied.
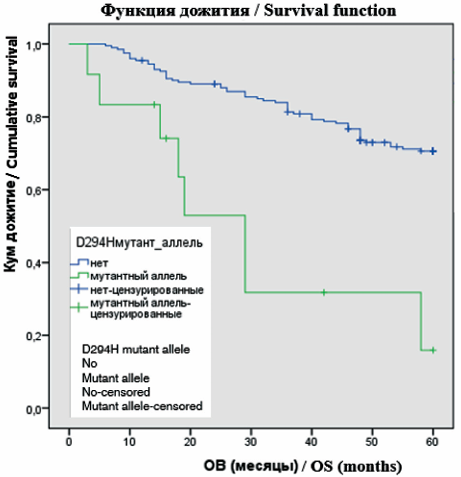
Objective: to comprehensively assess the associations of five key polymorphic variants of the MC1R gene (R151C, R160W, D294H, R163Q, I155T) with constitutional characteristics, primary tumor parameters, overall survival (OS), and event-free survival (EFS) in patients with CM.
Material and Methods. A single-center retrospective cohort study included 213 patients with primary CM at stages I–III. Genotyping was performed using allele-specific real-time PCR with melting curve analysis. The χ2 test, Fisher’s exact test, and Mann-Whitney U test were used. Survival analysis was conducted using the Kaplan-Meier method with the log-rank test; multivariate Cox regression was applied to identify independent prognostic factors.
Results. Specific phenotypic profiles were established: R151C was associated with male sex, skin phototype I–II, and a history of severe sunburns (p<0.05); R160W was associated with the “red hair/ freckles” phenotype (p<0.05). Carriers of R151C had tumors with greater thickness (p<0.001). The most significant differences were found in prognosis: carriers of the D294H and I155T alleles demonstrated the lowest survival rates. The five-year OS for D294H was 28.4 % compared to 66.7 % in the wild-type group (p<0.001). In the adjusted model, only D294H (HR=4.21; 95 % CI 1.92–8.97; p<0.001) and I155T (HR=3.72; 95 % CI 1.65–8.39; p=0.001) remained independent predictors of unfavorable OS. The influence of R151C on the outcome was mediated by unfavorable morphological features.
Conclusion. The contribution of MC1R polymorphisms to the course of CM is heterogeneous. The D294H and I155T alleles are independent determinants of an extremely unfavorable prognosis, while R151C serves as a marker of a high-risk phenotype and a locally aggressive tumor, and R160W determines only a constitutional phenotype. The data obtained justify the feasibility of integrating genotyping for the D294H and I155T variants into risk stratification algorithms to personalize follow-up for patients with CM.
LABORATORY AND EXPERIMENTAL STUDIES
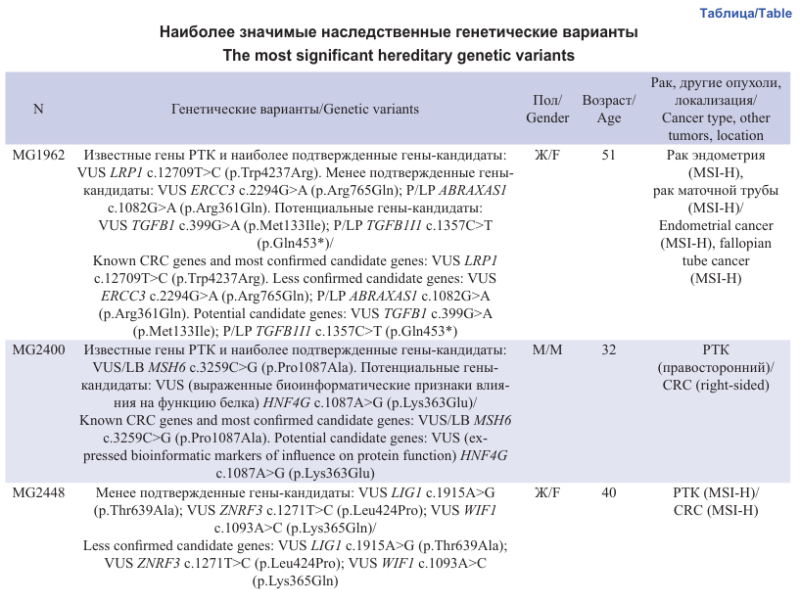
Aim: to identify new genetic causes of lynch-like syndrome (LLS), a hereditary tumor syndrome characterized by the development of neoplasms with high microsatellite instability (MSI-H) and the absence of mutations in known Lynch syndrome genes.
Material and Methods. The study included 18 cases of MSI-H colorectal cancer (CRC), endometrial cancer (EC), and gastric cancer (GC) in young patients without mutations in the MLH1, MSH2 (EPCAM), MSH6, and PMS2 genes. Whole-exome sequencing was performed on DNA from patients’ peripheral blood samples.
Results. At least one pathogenic or potentially significant/candidate genetic variant was detected in all cases (77 variants total). Most patients carried a combination of several potentially significant variants. The most significant finding was the identification of a FAN1 gene variant of uncertain significance (VUS) co-occurring with an EXO1 gene mutation in a young patient with MSI-H CRC. Digenic inheritance involving these two functionally related genes had been previously proposed as a hypothetical mechanism for LLS. Another case of presumed digenic inheritance was identified: co-occurrence of two VUS in the TP63 and TP73 genes, both predicted to be functionally significant by bioinformatics tools. A number of VUS and pathogenic/ likely pathogenic (P/LP) variants were found in candidate CRC genes: LRP1 (n=2), HECW1, PSME4, APCDD1, HIC1, CDK18, SMAD6, ZNRF3, WIF1, WNK2, RBBP8NL, MAP1LC3A. Several new candidate CRC genes are proposed: ST6GALNAC1, TGFB1I1, TGFB1, PTPRD, NUDCD2, WIF1, STAG3, NFATC2, HNF4G. Seventeen out of 77 potentially significant variants were heterozygous VUS or P/ LP variants in DNA repair genes: ABRAXAS1 (P/LP), FANCD2, BLM (P/LP), CHEK2 (hypomorphic mutation), RECQL4, BRIP1, ERCC2, ERCC3, XPC (P/LP), MUTYH (P/LP), UNG, REV3L, PARP1, PARP3, LIG1.
Conclusion. Whole-exome sequencing enabled the detection of potentially significant genetic variants in the studied patients. Verification of the clinical significance of the candidate genes and variants will be possible as epidemiological data continues to accumulate.
Circulating tumor cells (CTCs) are frequently studied in terms of their prognostic significance during perioperative systemic therapy (periST) for breast cancer (BC). it is not yet clear whether there are unique changes in the CTC parameters that could be used as a predictor of the effectiveness of neoadjuvant (neoST) or adjuvant (aST) systemic therapy.
The aim of the study was a comparative analysis of parameters of once-isolated CTCs in BC patients with high risk of progression, who received neoST or aST.
Material and Methods. The study included BC 39 patients who received neo-ST (group 1: 16 patients) or aST (group 2: 23 patients). Blood sampling for CTC isolation using microfiltration was performed after 2–5 cycles of periST.
Results. No significant differences in the number of CTC-positive patients (87.5 % in group1 and 82.6 % in group 2) and the frequency of isolation of 5 or more CTCs (37.5 % in group 1 and 52.2 % in group 2, p=0.563), as well as CTC clusters (56.2 % and 43.5 % of patients in groups 1 and 2 groups, respectively, p=0.646) between the neoST and aST groups were found. There were no significant differences in the quantitative parameters (Me) of CTCs between the groups (1 group – 3 [1.8; 7.8] CTCs, 2 group – 5 [2; 6.5] CTCs, p=0.785). Regardless of the group, most patients had CTC clusters consisting of 2 to 3 cells (88.9 % and 100 % of patients in groups 1 and 2, respectively). During peri ST, a high count of CTCs was associated with the detection of CTC clusters and the presence of lymphatic metastases.
Conclusion. No significant differences in CTC count and characteristics between the neoST and aST groups were found. it indicates that breast tumor resection has a minor effect on CTC parameters. . The findings highlight that CTCs hold similar prognostic value regardless of whether they are measured before or after surgery, aiding in the prediction of periST.
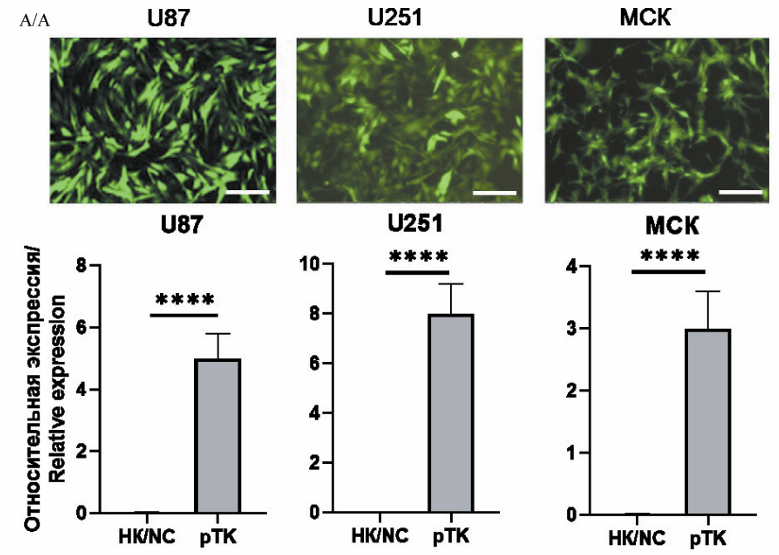
Background. Glioblastoma (GBM) is the most aggressive and malignant type of glioma, representing the most common and lethal primary central nervous system (CNS) neoplasm in adults. Despite current therapeutic approaches, the median overall survival remains low. Oncolytic virotherapy is a highly promising alternative strategy. One such approach utilizes the Herpes Simplex Virus Thymidine Kinase (HSV-TK) enzyme combined with the prodrug ganciclovir (GCV). This TK-GCV system is converted into a toxic metabolite that induces apoptosis in target cells. Combining the TK-GCV system with temozolomide (TMZ), the standard first-line chemotherapeutic agent for glioma, targets two critical survival mechanisms of GBM: DNA repair and apoptosis regulation. This combination has the potential to significantly improve therapeutic efficacy.
Aim. We evaluated the impact of combined TK-GCV and TMZ therapy on glioblastoma cell viability and migratory capacity in vitro.
Material and Methods. This work employed the following cell lines: GBM cell lines U87-MG and U251-MG, HEK293T/17 cells, and human mesenchymal stem cells. Recombinant viral particles encoding the thymidine kinase (TK) gene were generated using genetic engineering techniques. Optimal concentrations of TMZ and GCV were determined. Cell viability was assessed using the MTT assay; cell cycle distribution (G2/M phase) and Bax expression were analyzed by flow cytometry; gene expression was quantified via quantitative PCR (qPCR); and cell migration was measured using a wound-healing assay.
Results. The combination of TMZ and the TK-GCV system results in a significant increase in GBM cell death compared to monotherapy. Specifically, this enhanced cell death is characterized by a higher proportion of apoptotic cells. Furthermore, expression levels of EMT markers such as CD44, ZEB1, SNAI1, SNAI2, and VIM were significantly reduced under the combined treatment of TK-GCV and TMZ.
Conclusion. The combination of TK-GCV and TMZ demonstrates a synergistic effect between the two therapeutic approaches. Compared to each method administered separately, the combined treatment results in increased GBM cell death and reduced cell migration.

Preclinical studies of antimetastatic anticancer drugs require non-invasive monitoring of the metastatic process in live animals.
This study aimed to evaluate the efficacy of microCT and 18F-FDG PET/CT for imaging lung metastases in laboratory mice. These modalities were chosen based on the fact that PET/CT is optimal imaging modality for detecting secondary lung lesions in clinical practice.
Material and Methods. lung metastases of B16F10 melanoma were established in ten C57Bl/6 mice via intraosseous injection of a tumor cell suspension. On days 1, 7, 14, 21, 28, and 35 post-injection, the animals underwent “Accurate” CT of total body, followed by “Ultra focus” CT of the lung area. Based on the CT findings, three mice were selected for 18F-FDG PET/CT with iohexol contrast enhancement on day 38. Subsequently, the animals were euthanized, and metastatic foci in the lungs were confirmed by necropsy and macroscopic pathological examination.
Results. “Ultra focus” CT detected metastatic foci with a diameter of 0.4 mm and larger. PET imaging revealed moderate 18F-FDG uptake in lesions with a volume of ≥1 mm³ (SUVmax=2.8 ± 0.6). Foci smaller than 1 mm³ did not show significant radiotracer accumulation (SUVmax=1.6 ± 0.5). Contrast-enhanced PET/CT with iohexol clearly visualized the primary tumor node and allowed for the assessment of metabolically active tissue within it (SUVmax=3.4 ± 0.7).
Conclusion. integrated PET/CT does not provide significant advantages over standalone high-resolution CT for monitoring metastatic lung involvement in preclinical models. The modality of choice for the quantitative assessment of pulmonary metastases in small laboratory animals should be considered microCT. Contrastenhanced PET/CT may be utilized for evaluating the status of the primary tumor node.
ONCOLOGY PRACTICE
Introduction. Gastric cancer remains the leading cause of cancer-related morbidity and mortality worldwide and in Russia. In recent years, significant progress in treatment has been made through the use of modern neoadjuvant/perioperative therapy techniques. The grade of tumor pathomorphological response is a direct indicator of the effectiveness of neoadjuvant therapy, but the correlation between this response and long-term treatment outcomes varies significantly among different authors. The impact of a complete morphological tumor response on the patient’s treatment strategy and disease prognosis is a crucial scientific and practical challenge, and it remains a subject of debate.
Material and Methods. The study is planned as a multicenter, cohort, non-interventional, retrospective, open clinical trial. The studied treatment approach is neoadjuvant/ perioperative therapy followed by radical surgery for gastric and esophagogastric junction cancer in patients with complete tumor pathomorphological response after neoadjuvant therapy. The study is planned to include 200–250 patients who meet the following main criteria: morphologically verified gastric cancer (adenocarcinoma) and esophagogastric junction (Siewert III); clinical stage I–IVA, M0; neoadjuvant therapy (at least 1 cycle of chemotherapy) and radical surgery; pathomorphological stage of T0N0/N1–3. The primary endpoint (the main goal of the study) is to assess the 3-year overall survival rate. The total duration of the study will be 12 months. To analyze the treatment outcomes, an original database will be created using the Microsoft Excel 2010 program. Statistical analysis will be performed using the SPSS program, version 23.0. The study will be conducted in accordance with the principles of the Declaration of Helsinki, international and Russian rules for conducting scientific research in the field of medicine, and the legislation of the Russian Federation, and it has been approved by the Ethics Committee of the A.F. Tsyb Medical Research Center.
Results. For the first time in Russia, a multicenter retrospective clinical study will be conducted to assess the treatment outcomes in patients with locally advanced stomach cancer and esophagogastric junction cancer, provided that the tumor has a complete pathomorphological response after neoadjuvant therapy. The collected data (approximately 250 cases) is expected to be the largest in the world for this category of clinical observations. For the first time, representative data will be obtained based on the treatment outcomes of the Russian population of gastric cancer patients, including in real-world clinical settings.
Conclusion. It is expected that the results obtained during the implementation of this study will have both important scientific significance and practical application, including the possibility of using them in the national clinical guidelines.
Aim: to develop a model for predicting the risk of developing complications of rectal cancer treatment.
Material and Methods. A single-centre retrospective study included 302 patients diagnosed with rectal cancer, who were treated in 2017–2018 at the Yaroslavl Regional Clinical Oncology Hospital (YRCOH).
Inclusion criteria were: histologically verified rectal cancer and curative-intent radical surgery. The primary endpoint of the study was to identify factors influencing the development of complications. A binary logistic regression method was used to construct the model. The initial set of parameters for the model included the tumor differentiation grade (based on the primary biopsy), distance from the distal edge of the tumor to the dentate line, history of varicose veins of the lower extremities, diabetes mellitus, obesity, and the Charlson Comorbidity index. Seventy four rectal cancer patients treated in the YRCOH in 2019–2022 were studied as a test sample
Results. The resulting equation for the probability of developing complications of rectal cancer treatment was: р=1/(1 + e-y), where р is the probability of developing complications of rectal cancer treatment, y=0.52-0.54x1 - 0.1x2 + 2.3x3 + 3.4x4 , where x1 is the tumor differentiation grade (from primary biopsy), x2 is the distance from the distal edge of the tumor to the dentate line, x3 is a history of general obesity, x4 is a history of diabetes mellitus. The quality of the model turned out to be acceptable (p (Hosmer-Lemeshev)=0.68; pseudo-R2 Nagelkerke=0.53). At р>0.5, a conclusion was made about the high probability of developing cancer treatment complications. The prediction model was validated on a test sample of 74 patients. Thus, the sensitivity of the model was 82.35 % (95 % CI 73.2–94.9), the specificity was 97.50 % (95 % CI 82.2–99.9). The accuracy of the prognostic model was 89.33 % (95 % CI 80,0–99,5).
Conclusion. The model for predicting complicated follow-up in patients with rectal cancer will physicians to determine the likelihood of adverse events and take effective preventive measures.
REVIEWS
Objective: to evaluate the optimal timing of dental implant placement in cancer patients after jaw resection and reconstruction and to identify factors influencing their survival.
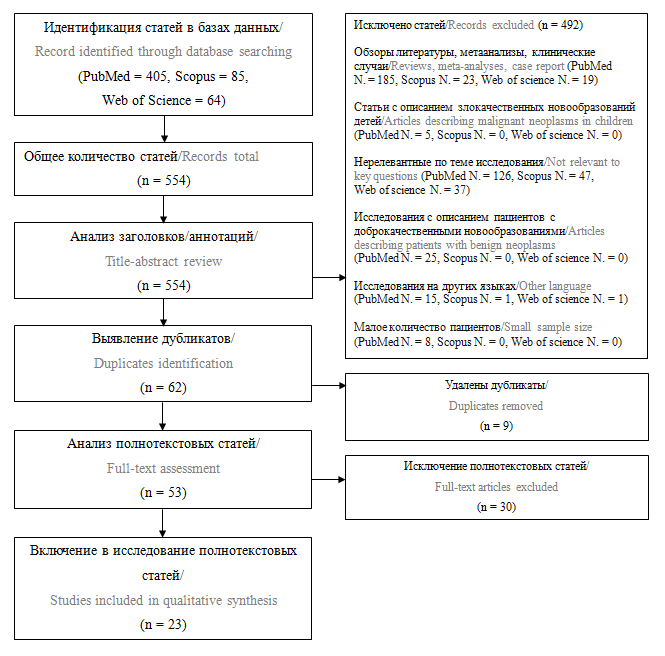
Material and Methods. A systematic literature search was conducted in MEDLINE (PubMed), Scopus, and Web of Science databases, including original articles published since 2000 evaluating dental implantation in cancer patients with head and neck tumors, who underwent jaw reconstruction using free vascularized bone flaps. The primary endpoint of this systematic review was dental implant survival in cancer patients. The secondary endpoint was the effectiveness of prosthetic rehabilitation, including the feasibility and success of functional prosthetic restoration. The initial database search identified 554 scientific studies, of which 23 were included in the final analysis.
Results. Based on the analysis of the eligible studies, the survival rate of dental implants in cancer patients who underwent jaw reconstruction using bone flaps varied widely, ranging from 44 % to 100 %. Moreover, nearly all studies demonstrated reduced dental implant survival in patients who had received radiotherapy.
Conclusion. An analysis of the literature showed that dental implantation in cancer patients who underwent jaw resection and reconstruction is a clinically justified and potentially successful method of rehabilitation. The survival rate of implants can vary widely, with prior radiotherapy appearing to be the most influential factor.
Study Objective: to provide an overview of current scientific data on the impact of H. pylori infection and eradication therapy on the development, clinical course and treatment outcomes of gastrointestinal cancer.
Material and Methods. A search of Russian and English-language literature sources published in various databases (MedLine, Pubmed, Scopus, The Cochrane Library, and Russian Science Citation Index) between 2004 and 2025 was conducted. Fifty-three available scientific publications were analyzed, including 5 Russian and 48 foreign publications, including 41 articles, 10 meta-analyses, and 2 retrospective studies.
Results. An analysis of scientific papers showed that H. pylori infection significantly worsened treatment outcomes and survival in patients with already diagnosed gastric cancer. Literature data demonstrate a positive impact of H. pylori eradication on survival in both early and advanced gastric cancer. In addition to being a major risk factor for stomach cancer, H. pylori infection is also associated with an increased risk of colorectal cancer, esophageal adenocarcinoma, pancreatic cancer, and biliary tract cancer. Furthermore, H. pylori infection impacts the effectiveness of immunotherapy in cancer treatment
Conclusion. H. pylori infection and eradication therapy can influence the development and clinical course of gastrointestinal tumors. Despite the close attention of many scientists to this issue, key questions remain poorly understood.
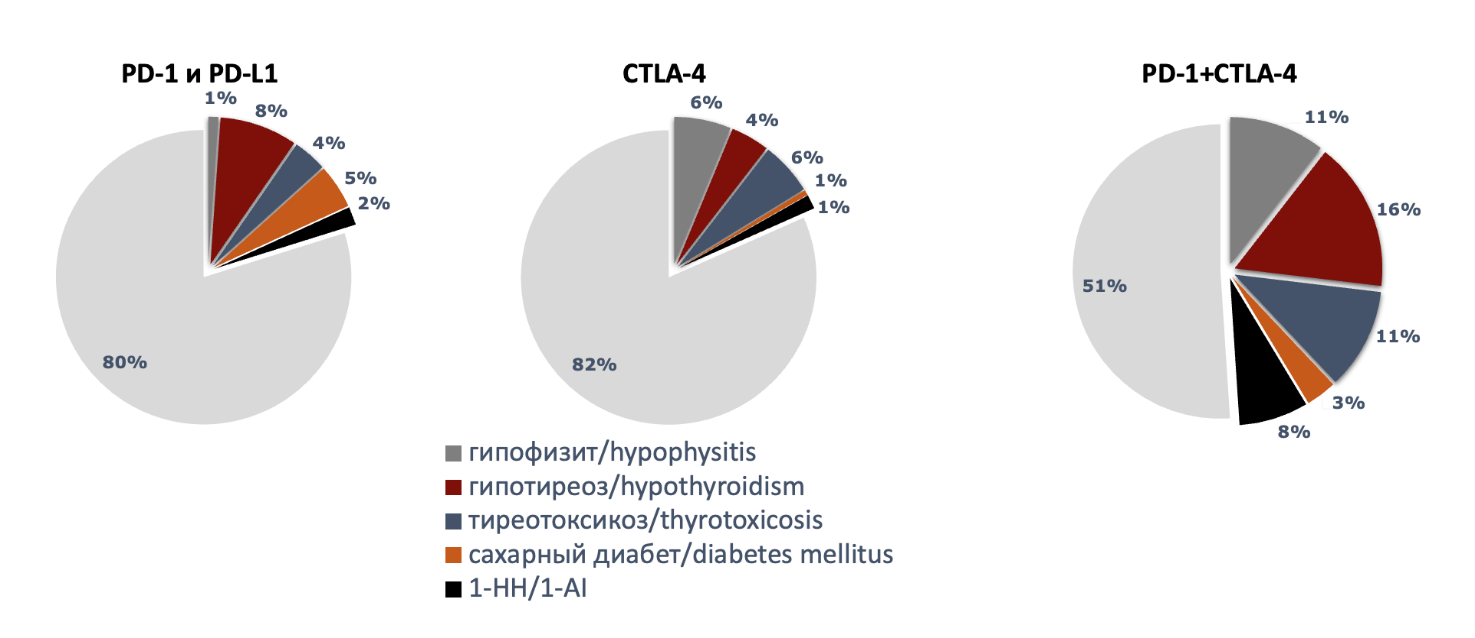
Objective: to summarize current data on immune checkpoint inhibitor-induced hypothalamic-pituitary-adrenal axis dysfunction, with an emphasis on hypophysitis and primary adrenal insufficiency.
Material and Methods. A review of publications on endocrine immune-related adverse events from anti-CTLA-4, anti-PD-1 and antiPD-L1 inhibitors was carried out from January 2015 to October 2025 using Pubmed, Cochrane library, Google Scholar, and Elibrary systems. Of the 876 studies found, 45 were used to write the systematic review.
Results. immune checkpoint inhibitor-induced hypothalamic-pituitary-adrenal axis dysfunction is a serious immune-related adverse event. It commonly presents as hypophysitis (particularly with anti-CTLA-4, causing pituitary deficiency) and primary adrenal insufficiency (risking fatal Addisonian crisis). Diagnosis is complicated by the nonspecific clinical presentation. Essential evaluation includes assessing symptoms, adrenocorticotropic hormone, cortisol, electrolyte levels, and hormones of other axes, as well as magnetic resonance imaging of the pituitary gland and computed tomography of the adrenal glands. in most cases, long-term, and sometimes lifelong, hormone replacement therapy is required.
Conclusion. Hypothalamic-pituitary-adrenal axis dysfunction associated with immune checkpoint inhibitor therapy remains underrecognized immune-related adverse event, requiring early recognition through clinician vigilance and screening algorithms to prevent adrenal crisis, improve quality of life and maintain cancer treatment efficacy. Multidisciplinary collaboration between oncologists and endocrinologists is particularly important in the care of these patients at all stages of treatment and follow-up.

Aim: to summarize the available literature data on the role of matrix metalloproteinases (MMPs) in angiogenesis, as well as in the development and progression of colorectal cancer (CRC).
Material and Methods. A literature search was conducted in the Medline and eliBRARY.RU databases from 1999 to the present using the keywords “angiogenesis + cancer + colon + MMP”.
Results. Malignant tumors are characterized by the ability to form new vessels, invade surrounding tissues, and metastasize to distant organs, and this aggressiveness depends on the expression of proteolytic enzymes, including MMPs. in CRC, the levels of MMPs are increased in both tumor tissues and blood plasma; these enzymes are required for extracellular matrix remodelling during angiogenesis, tumor invasion and metastasis. The degree of overexpression of certain MMPs correlates with the stage of CRC, vascularization, VEGF expression and/or prognosis; however, not all researchers agree with these findings. MMPs are synthesized both by tumor cells and, more prominently, stromal cells like tumor-associated macrophages. Alterations in the function of immunocompetent and stromal cells that express and produce MMPs play a key role in both the initiation and progression of CRC. Targeting tumor-associated immunocompetent and stromal cells, their reprogramming, neutralization and/or inhibition of their trafficking may delay the growth and invasion of CRC. inhibition of MMPs may represent one of the stages of antiangiogenic therapy. in addition to suppressing angiogenesis, certain MMP inhibitors stimulate apoptosis, suppress cell proliferation, induce cell cycle arrest, and reduce the expression of antiapoptotic genes of the Bcl family. A wide range of artificial and natural compounds and methods has been proposed as MMP inhibitors. However, despite promising experimental results, clinical trials of MMP inhibitors have been largely disappointing. There is evidence that some MMPs exert antitumor effects, and their blockade may be accompanied by tumor progression.
Conclusion. A wide variety of approaches to targeting MMPs, together with the certain inconsistency of available data, may indicate the persisting dissatisfaction of researchers and clinicians with the current solutions to the problem of MMP-mediated angiogenesis in tumor tissues. This also highlights the need for continued investigation into both the effects of MMPs in CRC and the methods for controlling the activity of this enzyme group.
The aim of the study was to study the effectiveness of combination of photodynamic therapy and immunotherapy in cancer treatment.
Material and Methods. We searched and analyzed 843 publications available from WoS, Scopus, MedLine and RSCI databases over the past 5 years. Out of 843 articles, 60 were included in this review.
Results. Preclinical and clinical data indicate the promise of combined photodynamic therapy, which is able to enhance the immune response and overcome resistance to PD-L1 inhibitors by destroying tumor vessels and improving antibody delivery. Photodynamic therapy is actively being investigated as a method of stimulating antitumor immunity, especially in combination with immunotherapy, turning “cold” tumors into “hot” ones. It promotes the growth of cytotoxic T-lymphocytes, suppresses regulatory T-lymphocytes and improves the interaction between tumor and effector cells, while disrupting regulatory mechanisms. Photodynamic therapy can also affect the expression of PD-L1/PD-1. Given the good tolerability of photodynamic therapy, its combination with immunotherapy can increase the effectiveness of treatment while minimizing the risks. Studies have shown that tumor mutation load and PD-L1 expression can predict treatment response in non-small cell lung cancer. In patients with lung adenocarcinoma with low/ moderate tumor mutation load and negative PD-L1, an improvement in overall survival was observed, which is consistent with data on the association of tumor mutation load with response to PD-L1 inhibitors. In the context of gastric cancer, the combination of photodynamic therapy with PD-L1 blockade has shown efficacy in restoring antitumor immunity by increasing the infiltration of cytotoxic T-lymphocytes and reducing the activity of regulatory T-lymphocytes.
Conclusion. The combination of photodynamic therapy and immunotherapy has great potential, as photodynamic therapy destroys cancer cells and stimulates the immune response, and immunotherapy complements and enhances this effect.
ANNIVERSARIES

OBITUARY

ISSN 2312-3168 (Online)










































